florida blue appeal form
Please describe the issue in as much detail as possible. Worthless Check Hardship Hearing Form.
2
Florida Blue Provider Disputes Department.

. Supporting documentation must be submitted. Complete Edit or Print Tax Forms Instantly. Request for Eligibility Review.
PO BOX 44197. Jacksonville Florida 32231-4197. BlueDental Choice - Form ID.
Accident Driver Exchange of Information. Blue Cross and Blue Shield of Florida. Mail the form and supporting documentation to.
4f4a45da30 27 claim form. Ad Access Tax Forms. To submit a prior authorization online please click the button below to use the web form.
To terminate the contract without providing a reason or offering an appeals process. Download Or Email Form DR-1 More Fillable Forms Register and Subscribe Now. Medicare Appeals and Grievances Department PO.
Amanda Flores on bluecross blueshield of florida appeal form. BlueDental Care - Form ID. Ad Access Tax Forms.
Use the e-signature tool to add an electronic signature to the form. Please describe the issue in as much detail as possible. Accordingly I authorize persons or entities that have any medical or other records or knowledge.
An application for payment of benefits under a health plan. Mail the form and supporting documentation to. The following tips will allow you to fill out Provider Appeal Form Instructions - Florida Blue quickly and easily.
Fill in the required boxes that are yellow-colored. Download Or Email Form DR-1 More Fillable Forms Register and Subscribe Now. Open the form in our feature-rich online editing tool by clicking on Get form.
I HEREBY request a review of the adverse benefit determination described below and understand the. Check the Adverse Determination box under Appeal Type. If necessary use additional sheets.
Complete Edit or Print Tax Forms Instantly. Get rewarded for healthy behaviors. Florida Blue Health Plan Appeals Jacksonville FL 32231-4197 Health Plan Grievance and Appeal Form I understand that in order for Florida Blue to review my appeal they may need medical or other records or information relevant to my appeal.
Self-insured Plans - Form ID. If necessary use additional sheets. Hit the green arrow with the inscription Next to move on from one field to another.
Box 41629 Jacksonville FL 32203 -16 29 Fax. Supporting documentation must be submitted. PPO Plan Appeal Form for use by Covered Persons with BlueOptions and BlueChoice Group Coverage and BlueOptions Individual Coverage Please mail directly to.
Check the Adverse Determination box under Appeal Type. Application for Formal or Informal review of Driver License. Application for Hardship or Administrative Hearing.
Discover all the ways members can earn wellness incentives and rewards for taking an active role in their health. Member Appeal and Grievance Form Mail to.
2

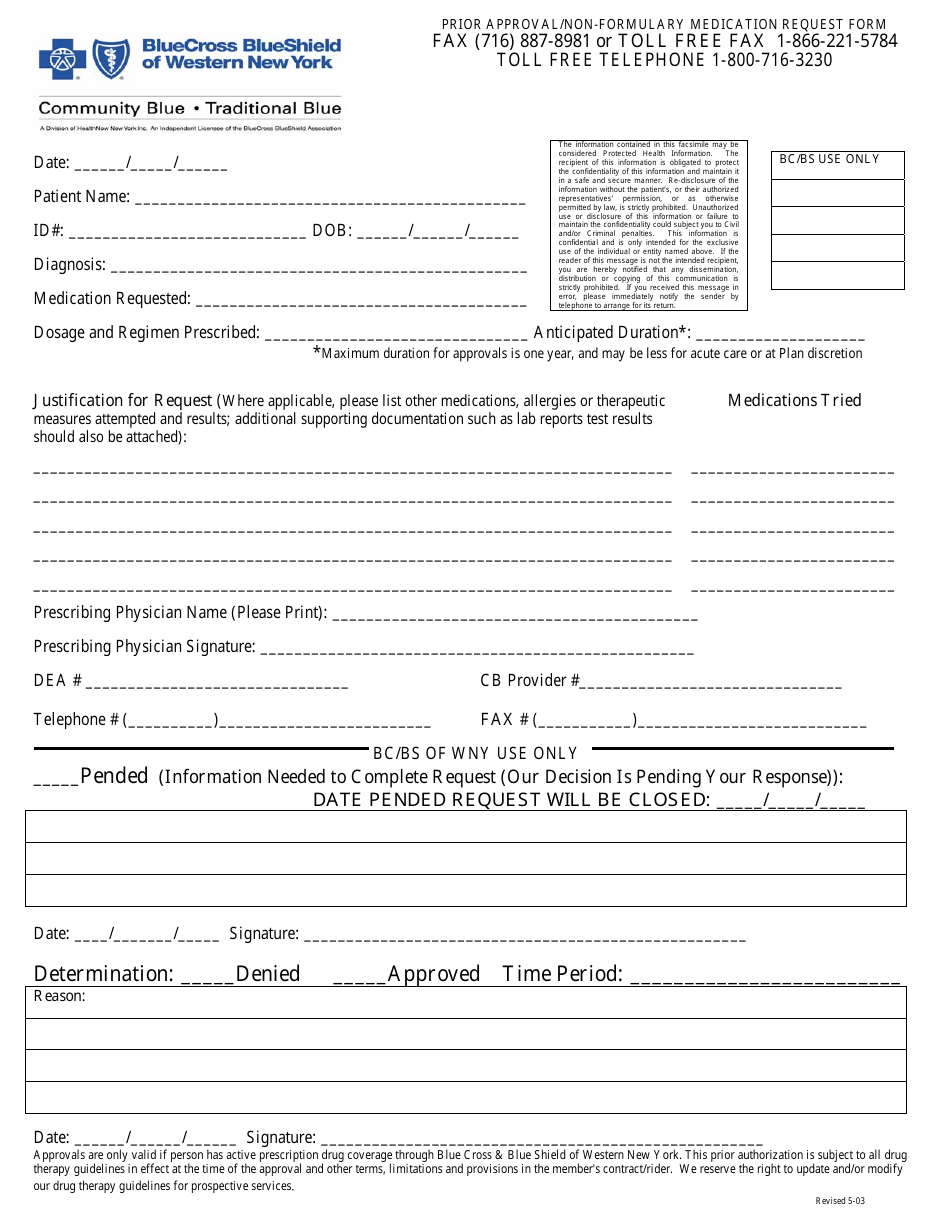
Free Prime Therapeutics Prior Rx Authorization Form Pdf Eforms
2
How To Write Convincing Va Statements In Support Of Claim Hill Ponton P A
2

Claims Denials And Appeals In Aca Marketplace Plans Kff

Blue Cross Blue Shield Prior Authorization List
Blue Cross Blue Shield Prior Authorization List
Blue Cross Blue Shield Prior Authorization List

Provider Appeal Form For Blue Cross Of Florida Fill Online Printable Fillable Blank Pdffiller
2
2
2
2
Get Our Example Of Medical Necessity Letter Template Letter Templates Letter Sample Lettering
2
2

Florida Blue Appeal Fax Number Fill Online Printable Fillable Blank Pdffiller

Blue Cross Blue Shield Prior Authorization List